The other day I was talking with a new client. It was our 3rd visit. Great guy. Super smart. Been in pain for about a year.
Meniscal surgery back in the Spring didn’t fix his knee pain. This is not surprising to me, as multiple studies have shown no difference in outcomes between people who get their meniscus repaired and people who have a ‘sham’ or fake surgery.
No difference in outcomes.
Take a look at this much replicated study in the New England Journal of Medicine.
Anyhow, back to creating your own luck. My new friend let me know that the moves we recorded for him to practice felt quite good (we use an app to record the moves and ideas we’ve come up with in each session to make it easy to remember). But after standing for 5 hours at work, his knee still hurt.
How often are you doing those moves that feel really good?
“I do about 10 of them in the morning.”
If you compare the amount of time you are doing things that contribute to the pain (standing at work, hauling brush in the garden, etc), multiplied by the year you’ve been experiencing this pain, to the amount of time you are doing those moves that make you feel good, what would the ratio be?
Remember, he’s super smart — an economics guy — so that’s all I really needed to say. If anyone is good with math, feel free to figure out the ratio for 5 minutes out of 24 hours multiplied by a year.
I’m a simple girl. I got my daughter’s 6th grade math wrong yesterday. What I do know is, we have to create situations for ourselves that will allow us to find luck 🍀
If you are at the point in life when one day your back is hurting and the next week it moves over to your shoulder, or the morning aches and pains are making you wonder what it’s going to be like in 5 or 10 years, I invite you to join the conversation. Send me a message or go to Facebook and search for the Private Group BeFIT NOW.
The ‘FIT NOW’ are those who reject what it used to mean to get old and stop measuring themselves by what they used to do easily in their 20s.
The FIT NOW create their own future by moving, doing, thinking, and believing differently in the present. This is the art and science of BeFIT NOW.
Relying on doctors, medicine, and healthcare to keep moving isn’t the fantasy. The fantasy is the lifestyle of complete freedom that being FIT grants.
The question is then, how can one achieve the complete freedom of an active lifestyle without planning it and doing it NOW?
Let’s do this together. Let’s BeFIT NOW because later doesn’t get us where we want to be.
You know those days when you are too tired to focus, too busy to feel in control, too {insert something frustrating} to enjoy {insert something great}?
What if the thing that turned that around was to be a little selfish?
That sounds crazy, but stick with me. This advice, to be selfish in order to get your personal energy out of the hole — in order to then become more open and generous — is given 44,000 times a day, to 2.7 million people, across 29 million square miles of space.
Airspace.
Every flight you’ve ever taken starts with a survival lesson about being selfish before you can be of use to anyone else.
Put your mask on first.
There are 44,000 flights every day, carrying 2.7 million people, across 29 million square miles around the globe — all hearing this message: In event of emergency, make sure you are breathing before trying to help anyone else.
Back on the ground, we encounter countless big and little emergencies all day. The question is, are you securing your own mask before attempting to help others?
Setting ourselves up to have the energy, and frankly the desire to be generous with our family, friends, co-workers, strangers, etc. means taking care of ourselves first. Even when we have company, when there is a deadline, when someone is sick, when we are traveling…
I’d say, those are the times when being consistent with the things we know give us energy is MOST important. It’s a feedback loop.
I can have a bigger impact if I build four areas into my day. Mindset, movement, nutrition, and recovery. I don’t see it as making time for these things, I just do my best to build them into my day.
Mindset: Personally, I love starting my day with the Headspace App. 10 minutes, at 5:00AM and I’m clear, creative and smiling before getting out of bed.
Movement: I’ve spent 25 years as a Physical Therapist working with amazing clients, learning, asking questions, evolving businesses, and teaching (with the Gray Institute).
This Two Minute Routine, adapted from my work with the GI, is hands down the most valuable and efficient series of movements I’ve ever seen put together.
I do this first thing in the morning and several times a day. If we want to move freely and enjoy the things we love for a long, long time… we have to invest in it.
Nutrition: I am NOT a nutritionist. There are many nuances better left to the experts. Personally, I like to keep things simple so that I don’t get overwhelmed. Eat more real food and less stuff that comes in packages. The fuel we put into our cars matters… so does the fuel we put in our bodies. Starting the day with protein and fruit works for me, then I’m more likely to continue with better choices as the day goes on.
Recovery: 7 to 8 hours on weekdays and 8 to 10 hours on weekends keeps me in balance. Vacations and little bits of time spent with my family remind me what I’m doing all this work for. Reading first thing in the morning allows me to ‘recover’ before the day even unfolds. Going on walks with my lady, who is my sounding board, my love, and often my much needed voice of reason.
If you often find yourself feeling too busy and are ready to change that, I invite you to join the conversation. Send me a message or go to Facebook and search for the Private Group BeFIT NOW.
The ‘FIT NOW’ are those who reject what it used to mean to get old and stop measuring themselves by what they used to do easily in their 20s.
The FIT NOW create their own future by moving, doing, thinking, and believing differently in the present. This is the art and science of BeFIT NOW.
Relying on doctors, medicine, and healthcare to keep moving isn’t the fantasy. The fantasy is the lifestyle of complete freedom that being FIT grants.
The question is then, how can one achieve the complete freedom of an active lifestyle without planning it and doing it NOW?
Let’s do this together. Let’s BeFIT NOW because later doesn’t get us where we want to be. Join our Private Facebook Group.
It depends. In fact only 5% of people with back pain need an MRI or CT to investigate a serious problem. Flip that, and we know 95% of people with back pain don’t benefit from images. So what’s the harm in checking? You may be surprised by the answer.
We’ve all said it, “a picture is worth a thousand words” and in most cases, I agree. Our minds can conjure up entire novels from one photo. Art can inspire generations to think and feel and do amazing things. Shouldn’t a high tech picture of our spine speak volumes about back pain? Time and again, science and experience tell us the answer is no.
The power of an image is undeniable, but the value of high tech diagnostics are under scrutiny. Photo by Juan Di Nella on Unsplash
It makes sense that if we have back pain and the technology is available, we want to see what’s going on inside. The temptation is strong for many practitioners and patients alike. Let’s get that picture to tell the story, have the doctor fix it and move on to bigger and better things.
This is where countless people have been lead down a long, rough road.
The vast majority of back pain is musculoskeletal — meaning an over-use or under-use of the muscle, connective tissue, and cartilage. It is movement related pain. This is something the literature has been clear on for years. Unfortunately, it’s still being treated like a disease that requires highly advanced medicine to detect and fix. Conservative management even sounds boring.
The solutions with the best results and least risk are low-tech and take some effort. It’s appealing to think pain can be fixed my medicine. As a result, common sense solutions don’t get much attention in modern medicine, advertising campaigns, or the media. As a Physical Therapist of 20+ years and ever curious person, I’m in the camp that believes simplicity is the key. Several years ago I did a talk for a group of practitioners from around the world titled, The Power of Know. As often happens, a Steve Jobs quote was central to the main idea:
Simple can be harder than complex: You have to work hard to get your thinking clean to make it simple. But it’s worth it in the end because once you get there, you can move mountains.
If you feel good, you can also climb mountains. Outcomes are what matter. If you feel good, you can golf, walk, run, pick up your kids and grandkids — you can live.
Take Linda for example. She’s a very young 70 year old artist with a sharp wit and kind heart. Her stories are nothing short of fantastic. Linda had low back surgery several years ago and came to see me in hope of some relief before her next one. Her surgeon said another fixation was the only way to stop the pain that has been gripping her back and traveling down her left leg for months. A second surgeon recommended physical therapy, “when that doesn’t work, we can do the surgery.” Perhaps not the best endorsement for the conservative approach.
She brought her MRI and CT for me to look at as we discussed her situation. I know Linda, I’ve been to her home for dinner. She asks about my girls and tells me I’m doing a good job with them. This is the kind of person Linda is. She’s in pain, can’t enjoy what she loves doing, yet still asks about my family.
I take a look at the MRI, though I already know what it’s going to say. The CT, apparently taken on the same day — not sure why both were done, perhaps because her insurance would cover it and both machines were right there in the office— gives the same information. There is a surgical fusion and decompression at L4/L5, now the joint above [L3/L4] is being over stressed. It shows an S curve in her upper back (scoliosis), which is evident by simply looking at her posture. The disc in the space between L3/L4 is bulging from the pressure and encroaching on the nerve that branches from that level. This is happening because the joint below [L4/L5] can’t move anymore, and the curve in her upper back is creating stress from above.
Many surgeons will mention in passing that in a few years you’ll probably be back for another fusion— ‘no worries, we’ll fix that too.’ I am not implying that all surgeons are walking around twirling their evil mustaches. There are plenty of docs openly speaking out about the low success rate of spinal fusion, which is 25–35%. Placebo effect is arguably somewhere between 25–50%. I’m not a math genius, but those aren’t good odds for the risk of surgery, the prevalent complications, and the high chance of needing another one in a few years.
In 1993 Dr. Gary Franklin published a paper showing that the return-to-work rate in the state of Washington after a spinal fusion for back pain was 15 percent. In a two-year followup, the return-to-work rate was 22 percent. Dr David Hansom, an orthopedic spine surgeon says those results got his attention.
“And then I looked at my own results. I looked at that data and I just stopped, because I realized that the fusions for back pain were not doing well.
Then about the same time a lot of my patients that had had fusions started breaking down above and below their fusions and a lot of patients became referred to me for breakdown above and below their fusions. And those are real problems. Those don’t do well without surgery.”
We can do better. We must do better.
After hearing Linda’s story, I asked if we could take a look at how she’s moving. “Has anyone watched you move?”
“No.”
“Did anyone show you what you can do to open up that space where the disc is under all that pressure?
“No…can you really do that?”
You may think this is unusual. To be told surgery is the only answer even though none of the experts in Linda’s care had watched her move. Even worse, to be given no strategies to relieve the pressure causing the pain.
This is the norm and it’s a shame.
No Disc is an Island
Discs don’t bulge because they feel like it, or they are inherently faulty. Discs are firmly attached to the vertebrae and are constructed brilliantly to absorb shock. They are part of the human ecosystem.
They don’t slip out of place. They bulge when ‘abnormal’ forces are exerted on them over time. If they don’t find a nerve to hit, the bulge doesn’t cause a problem. The factors contributing to stress are the problem and they can be addressed. The stress can be physical, social or emotional — most likely a combination of the three. Think ecosystem, not island.
Even if a disc is painfully bulging into a nerve, it can be resolved without surgery. In addition, “the risk of subsequent catastrophic worsening without surgery is minimal.” The New England Journal of Medicine published a study that definitively shows a protruding disc can resolve with the right conservative management (there’s that boring phrase again, let’s call it changing the ecosystem instead).
Fig. A shows severe nerve root compression of a 29 year old woman. Fig. B is the same woman 5 months after choosing physical therapy over surgery.
Often when surgery is done to fuse the vertebrae, nothing is done about the surrounding ecosystem that caused the problem in the first place. It’s like putting an old beach house on stilts even though the water is still eroding the beach and the next hurricane is only a matter of time.
After doing a movement assessment (3DMAPS) with Linda, it was clear where to begin. Her scoliosis isn’t fixed — meaning it changes with movement. Her hip motion is tight in some key areas, which the low back doesn’t like. We needed to teach her three moves to relieve the pressure. It’s not rocket science, it’s functional biomechanics. Unfortunately, there are very few practitioners who understand how to apply it.
I showed Linda the three moves, we recorded them on the mobile app we use to communicate with clients so they’d be on her phone. We did some soft tissue work through her hips, legs and upper back on the table. Linda left feeling confident about what she could do on her own and with us in the studio. That’s always the mark of a good first session, you should leave feeling more confident.
Another observation worth noting here is what happens to the paraspinal muscles after lumbar fixation. Along the incision, there is almost always a 2″ to 3″ long divot where the paraspinal muscles have denervated and atrophied. I see this over and over when working with people a year or more after surgery.
These are the deep paraspinal muscles that often become denervated and atrophied along the incision following spinal fusion.
Surgeons don’t seem to be concerned with this loss of nerve connection and resulting muscle atrophy surrounding the surgical site. I’ve never had a client who was aware of it before we discussed it. The literature on paraspinal muscle atrophy following lumbar surgery is minimal. We definitely know it happens a lot. One study says it probably has detrimental effect. Common sense would say that if the muscles directly attached to the bones don’t work anymore, then that’s not good. Sometimes you don’t need a study.
Another finding on Linda’s MRI was anterolisthesis of L3 on L4. That means an anterior or forward ‘list’ of one vertebrae on another. A reasonable hypothesis would be, if the paraspinal muscles are damaged after surgery, there is a greater chance of instability in the surrounding joints. Add onto that, therapy or exercise that doesn’t address the asymmetries (ecosystem) that caused the problem in the first place and we’ve got another storm on the way.
On her second visit Linda came in laughing and shaking her head. She’d not had any of the spasms or the aching pain down her leg that had been with her for months. As of this writing, it’s been 6 weeks since Linda’s first session and she’s doing very well. By that I mean she’s playing 9 holes of golf when she wants to and has had a chance to investigate her options in relative comfort.
“I’ve had PT so many times that didn’t do any good, the surgeon said I need surgery to fix it, and now I’ve had almost two months without that awful pain.”
We are not out of the woods yet. There are longstanding patterns in her body that will take over if she doesn’t continue to create new pathways of movement. Soft tissue work is also helpful in getting good circulation and clearing painful inflammation.
Some would call this pain management. I don’t like the negative conation of that term. She is rebalancing and redistributing the forces going through the disc at L3/L4, making is less likely for the nerve to be hit, and that is taking the pain away. She’s changing the ecosystem. It’s not rocket science, it’s functional biomechanics mixed with the confidence of going from a state of vulnerability to empowerment.
She has options and actionable information. She’s in significantly less pain, and therefore in a better position to make informed decisions. In the end, we all make our own choices and the more we know, the better.
I’ve given her a copy of Cathryn Jakobson Ramin’s book, Crooked: Outwitting the Back Pain Industry and Getting on the Road to Recovery. Ramin is an investigative journalist who’s experience with back pain led her down the rabbit hole. The five page bibliography alone is better than any Google search. We bought ten copies to loan out and pass on.
Back pain is not the unsolvable enigma it’s been made out to be. I learned how to interpret and apply principles of physical, biological and behavioral science at the Gray Institute after 15 years of practicing physical therapy. I’ve had the great opportunity to teach for them since 2013. The more practitioners that take the time to understand the why behind the what the better.
Dr. Gary Gray and Dr. David Tiberio of the Gray Institute are the pioneers of Chain Reaction Biomechanics. For over 30 years they’ve been humbly seeking to better understand the human ecosystem in the field of Applied Functional Science (AFS).
We’ve been trying to fix things that aren’t broken
There are normal changes that take place inside the body over time. These normal changes show up on MRI, CT and X-ray to take the blame for crimes they didn’t commit.
Research and peer review articles have been clear for years. Do an MRI or CT when there are neurologic signs and symptoms — like loss of bowel and bladder function. Otherwise, you may be doing more harm than good.
Modern medicine runs on a high tech, diagnose and treat mentality. Atul Gawande’s 2015 New Yorker article, Overkillis a call to common sense action.
The phenomenon of over-testing, [which] is a by-product of all the new technologies we have for peering into the human body. It has been hard for patients and doctors to recognize that tests and scans can be harmful. Why not take a look and see if anything is abnormal? People are discovering why not. The United States is a country of 300 million people who annually undergo around 15 million nuclear medicine scans, 100 million CT and MRI scans, and almost 10 billion laboratory tests. Often, these are fishing expeditions, and since no one is perfectly normal you tend to find a lot of fish.
What’s the harm in ordering an MRI or CT to diagnose back pain? The science (and the outcomes) are consistent in showing one thing – in the absence of neurologic impairment or history of cancer, the scans add nothing but cost. Real people are paying the financial, social, and emotional price.
The general public has no idea that the literature very rarely indicates the need for MRI or CT to diagnose and treat low back pain. So many people get them, that everyone knows someone who’s had an MRI for musculoskeletal pain. It’s engrained in our conversations and in our culture. The results of these costly tests leave countless people no closer to an answer than when they started. What they do is wrongfully leave you with a sense that your back is damaged and vulnerable.
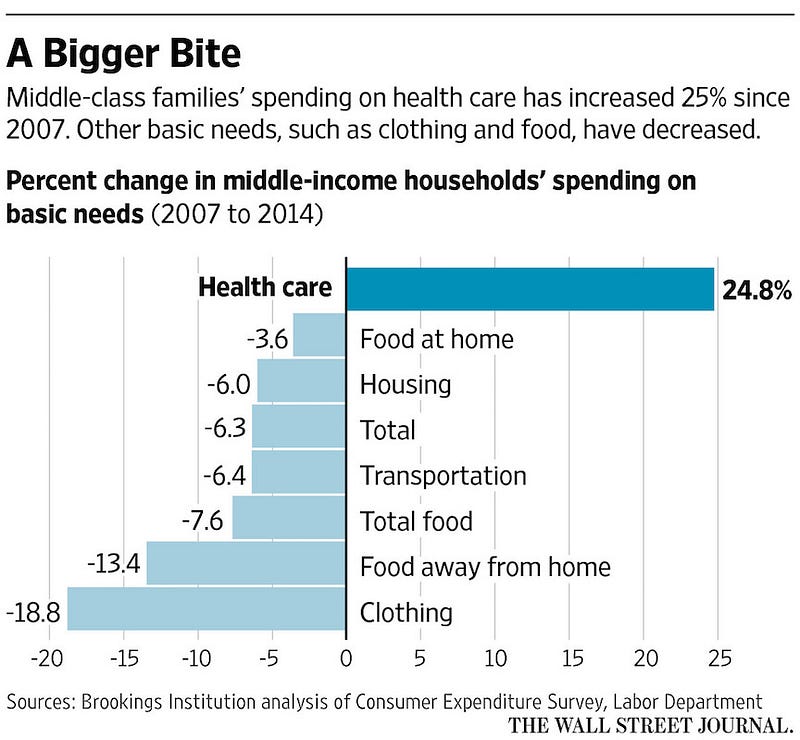
The unneeded scans (average cost is $2611) often lead to an avalanche of treatments with low to no value. We are spending upwards of $3.3 trillion a year on health care. Economists would blame (surprise!) economics. A reasonable economic explanation for the excess of low value care is the combination of fee for service and third party payment. Providers are paid more for doing more, while insurance foots most of the bill.
In reality, the patient and their employer are paying with the annual rise of premiums and deductibles to cover the previous year. Premiums have doubled every eight years for the past four decades. The rising cost for the fishing expeditions Gawande refers to is completely out of proportion to other basic needs. If we were getting better results the cost wouldn’t be under such scrutiny.
We can do better
While the economists have a valid point, it’s only one piece of the puzzle. According to the Archives of Internal Medicine, roughly half of the physicians polled said their patients received too much medical care. Too much doesn’t just imply wasteful care, but also harmful care. Many doctors point to ‘defensive medicine’, a phenomenon brought about by the fear of being sued or wracked with guilt if they miss something.
I think of our third party payor system as an open bar problem. An open bar feels free. On someone else’s dime, it’s top shelf all night. Maybe two drinks at a time to avoid waiting in line. At the end of the night it’s spills, and empty tables cluttered with 1/2 full drinks.
Imagine ‘free’ drinks and the bartender being paid more for every drink served. Yikes! That’s pretty close to fee for service care in a big medical system with a third party footing the bill. While economic incentives matter, there is a fundamental flaw to in trying to blame the entire problem on fee for service and third-party payments.
None of that would matter if the general public didn’t believe in the value of the service. Not only do we believe in it, since we pay the high premiums, we deserve it. Of course we deserve to be cared for compassionately and competently. The question is, when do we really need medical care and when do we simply need to change a few behaviors? In other words, when is it medical and when is it functional?
Dr. H. Gilbert Welch, an academic physician and professor at Dartmouth Medical School, is a heavyweight in the fight to bring awareness to the dangers of over-diagnosis and excessive medical testing.
“The general public harbors assumptions about medical care that encourage overuse. Assumptions like it’s always better to fix the problem, sooner (or newer) is always better, or it never hurts to get more information.”
When we start to talk about saving money and thinking twice about getting diagnostic tests, it gets…uncomfortable. Emotions run high. It’s not about saving money, denying care, and putting people at risk. Think less medicine and more health. It’s about common sense, informed decisions, and awareness of actionable options.
When it comes to our health and that of our kids, parents and loved one’s, it’s the outcomes that matter. More treatment is not always better. The outcomes of high tech testing and procedures — particularly with musculoskeletal issues — mean more medicine, not necessarily better health.
It goes without saying, we want the best care for ourselves and our loved one’s. The problem is, it’s increasingly difficult to filter out the noise and confidently know what’s best. Dr Hansen’s experience as a surgeon who has chosen to do less surgery is particularly interesting:
“So it’s actually fairly unpleasant to tell a patient who is demanding surgery — that you can’t do surgery, number one. Second of all, doctors do get paid well for doing surgery. We don’t get paid well for not doing surgery. So the patient’s demanding surgery. The hospital system is demanding production, which means more procedures, but also the patient’s themselves would rather have something done to them than to do something for themselves, like do solid rehab, etc.”
Back pain is a $100 billion industry in need of disruption
The source of the majority of back pain is musculoskeletal in nature and not detectable on an MRI or CT. We find the cause within your story and in the way you move (look for a practitioner certified in 3DMAPS). Your doctor or therapist should be a skilled and attentive interviewer. Questions like, “how can I help you?”, “what’s been going on?”, and “tell me more about that…” can reveal more than any diagnostic test.
Daniel Cherkin, a back pain specialist at the Kaiser Permanente Washington Health Research Institute says, “[Back pain is] not the only thing that’s been overmedicalized, but it’s probably the poster child for how things can go wrong in terms of patient outcomes and cost to society.”
Discs degenerate. Sometimes they bulge. At times they even protrude. These so-called abnormalities get a bad rap. They exist in as many people in pain as not. When they pop up in a high tech fishing expedition — often after years of being there, doing no harm — it’s assumed they must be the cause.
It’s no surprise that our skin looks different at 20 than it does at 65. We see our skin with every glance in the mirror. It’s in our face everyday, which makes it easier to accept as a ‘normal’ sign of a life being lived. We can’t see what’s under the skin, so we rely on the experts to analyze the pictures and let us know what’s normal and what’s not.
Discerning what is an unavoidable process of aging vs. a disease process should be the headline of every image report. For example, Degenerative Disc ‘Disease’ is a misnomer. Disc degeneration is a normal process that begins in our 20’s. It is not a disease and it does not cause pain. It’s old school science for a practitioner to think a degenerated disc causes pain.
Dr. Gawande says, “our ever more sensitive technologies turn up more and more abnormalities — cancers, clogged arteries, damaged-looking knees and backs — that aren’t actually causing problems and never will.’
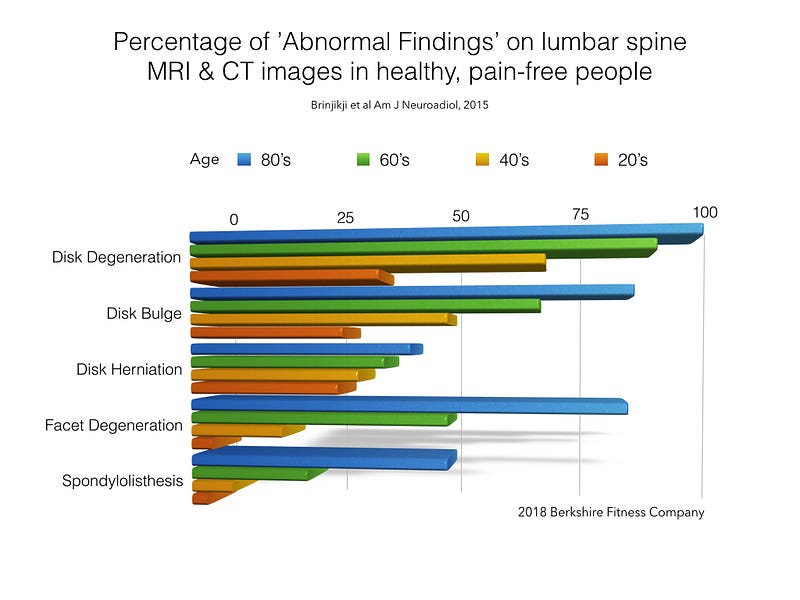
Results from a literature review of thirty-three studies with 3110 pain-free people.
These so called abnormalities exist in significant numbers of healthy, pain-free people of all ages. They are there whether we have pain or not. The graph above shows results from a 2015 Systematic Literature Review of Imaging Features of Spinal Degeneration in Asymptomatic Populations. Literature reviews are great because they look at multiple studies to find common ground. This one looked at thirty-three articles reporting imaging findings for 3110 pain-free people.
We can see that 37% of pain-free people in their 20’s have disc degeneration. It’s natural. 50% of pain free people in their 40’s have a disc bulge, and 36% of people in their 50’s have a disc herniation. It’s worth saying again, these are people without any pain.
If a herniation encroaches into a nerve space, there will be pain along the path of that nerve. The good news is, if you are working with someone who understands how the body moves, it’s likely they can help you open that space and relieve the pressure naturally. The same approach works for stenosis — the narrowing of the spaces that house spinal nerves.
Harvard Medical School agrees that Physical Therapy is just as good as surgery and less risky. Surgery should be avoided, especially when the success rates hover around 30% and the risks are high. A recent Johns Hopkins study found that medical errors are now the 3rd leading cause of death in the U.S. Too much medicine, not enough health.
It’s clear in the literature that images for non-neurologic back pain lead to over-diagnosis. This occurs when so called abnormalities are diagnosed as the source of the pain. We know degenerative discs are not painful. Remember, a disc is not an island, it’s part of the human ecosystem.
We know a large percentage of the population is walking about with bulges and herniations that do no harm. We know that even if the disc has protruded into a nerve it can recede naturally if the forces causing it to disperse are redistributed. We know enough about human movement to teach anyone how to do it.
As Steve Jobs said, it takes effort to get your thinking clean, but once you do it’s worth it. Not only can we move mountains, we can climb them if we want to.
A functional dynamic systems approach to musculoskeletal pain and discomfort is essential. The cause depends on our unique circumstances and experiences. The answers lie in the details of our stories and what we are willing to see and change— not in a single, static snapshot of our insides.
So when is an image the right thing to do?
There are a few red flags that you and your doctor must attend to. Loss of bowel and bladder function, loss of muscle control, and loss of feeling. Depending on your history and presentation, there are other valid reasons for testing. In Linda’s case, since she already had a spinal fusion years ago, it was probably a good idea to get an MRI based on her symptoms. We know after spinal fusion, the chance of instability above and below exists. I would still argue for the right conservative approach before jumping back into surgery.
In the same vein, as a PT, I’m fully aware that all physical therapy is not created equal. Use your judgement and don’t be afraid to ask why your PT chose a particular exercise or strategy. They should be able to give clear and concise explanations. Also be wary of clinics that do too many modalities (heat, ultrasound, electric stimulation) and not enough skilled investigation.
Good health care is like any good relationship. You should always be able to have an open and honest discussion with your doctor or therapist. The more a practitioner knows about you the better. The more interest they show in you, the better. If you feel like you aren’t heard, find someone who listens. Technology has made it possible for us to build relationships across the miles — both personally and professionally. We use encrypted technology for secure online consultations.
If the red flags aren’t flying, there are three questions to ask any practitioner who recommends an MRI, CT or X-ray for back pain:
Will it tell you something you don’t know already based on my history and current situation?
Does the research support the need for imaging to inform my treatment?
Will this test improve the quality of my life?
If the answer is no, or the practitioner struggles to find a clear answer, you’d do well to get a second opinion.
First’s hold a special place in our memories.
The first time you held your person’s hand.
The first kiss.
The first taste of a new city.
The first look on the kids faces when they see the presents under the tree…
These moments seem to suspend time and become etched in us. I listened to the most wonderful meditation the other day. It reminded me of the freedom of what Zen Buddhism calls ‘Beginner’s Mind’.
Most of us walk through the day silently (or not) casting our views and opinions out onto just about everything and everyone. Even — perhaps especially — those we are closest too.
It’s so easy to focus on a noise someone makes, a habit that annoys us or cast judgment on their actions. Maybe we waste all the wonder on the new, leaving what we have — and once longed for — feeling stale.
That meditation reminded me that my partner and I spent the first couple of years getting to know one another from opposite ends of the country.
Time together in the same city was precious. So full of curiosity. So new. So exciting and without hint of judgement.
What a gift.
There was a song I had on repeat during many of those days apart. One line sticks in my head:
“What I’d give to make you coffee… find out how you like your eggs.”
When you are apart from someone you love, a line like that can gut you.
Now we get to wake up everyday for coffee together AND she makes my eggs without fail every morning. It’s the simple things, that if I’m not careful to open up my ‘Beginner’s Mind”, I might forget.
So with ‘Beginner’s Mind’, I hereby re-enter into the craziness of Christmas and the Holidays with..
A little more gratitude while wrapping my kids gifts… and little less worrying if I have everything.
A little more anticipation of them tearing off the paper… and less stress about what else ‘needs’ to be done.
A little thought about how awesome it is to go cut the tree down with my girls, strap it on the car ourselves, cut the limbs off the bottom, and enjoy the beautiful lights… and a little less annoyance at the mess it might make.
A little more awe at the fact that I have a good business and we meet and help the most wonderful people everyday… and a little less stress about closing for the Holiday week.
And finally, a lot of laughter… and a lot less distraction.
“Me neither,” Violet said, “but if we wait until we’re ready we’ll be waiting the rest of our lives.” — Lemony Snicket, The Ersatz Elevator
I was standing on the porch of the tiny green house my daughter’s and I had only just moved into. My head was spinning. My heart was racing. The voice inside me was saying just do it. But then, “I’m not ready. I can’t possibly pack up and move again. We’re just getting settled. What the fuck am I thinking….”
In the preceding months, I had left a marriage that needed leaving. The girls and I regrouped and recouped for a couple of months at the home of my childhood best friend. Meanwhile the other amazing women in my life helped me make a cozy little home out of this weird green box. As the realtor had driven us up to it, the only real option in our town on my current budget, I remember thinking, “Oh God, don’t let it be that one.”
But now I kind of liked it and was standing on it’s postage stamp porch about to make another very big decision I clearly wasn’t ready for. The head spinning and stomach churning was the result of three things that had happened that day (never underestimate the power of three’s, especially when they hit you all at once).
One — the owner of the small private practice I had been contracting with had rather unceremoniously told me it was time for us to part ways. My side of that story has to do with his big ego and know-it-all style. I’m sure his side is quite different, but isn’t that always the case?
Two — our house, the one before ‘the leaving of the marriage’, went under contract. That meant I could get my equity, pay off the debt I had rung up after taking the leap, and maybe — just maybe — breathe again.
Three — a phone call from a friend, offering to partner with me on a new business six hours away in Western Massachusetts. I had just hung up the phone with him and was running through the incredibly timed conversation in my head. “I just spent an entire flight across the country thinking about how I could get you to move out here and do this,” he said, “so I had to call…”
Was I ready? Hell no. Did we do it anyway? Damn right.
That was July of 2015. We scrambled and moved to Williamstown the last week in August, and the girls started in their new school after Labor Day. Today I am 4 years into a successful and growing business. I have a wonderful partner who makes me laugh and think and loves me and my girls.
Had I not taken that opportunity, I’m not sure where we’d be right now. What I’m quite sure of is, had I not ‘started before I was ready’, I’d have regretted it.
I would never describe these last four years as easy. It’s not supposed to be easy. When I look at the strength and humor and wisdom my teen daughters now have — I know unequivocally that I made the right decision.
All progress begins with a brave decision. –Marie Forleo
These days, I see opportunities in everything. I’m not afraid to jump in to a project and make mistakes, because I know it’s the only way toward the next best thing. When I feel myself overthinking something, I take action. Action spawns courage, not the other way around.
So whatever it is that kept you reading today — whatever the next thing is for you (starting to exercise, taking that course you’ve been thinking about, fixing a relationship worth fixing or letting go of one that’s no longer healthy…) take a step. Sign up for the class. Send the email. Pick up the phone. Lace up your sneakers.
Bodies in motion tend to stay in motion.
I had the opportunity to give a talk on my experience with radical change in 2015 at Gray Institute in Adrian, MI.
Robin Dufour: Things Have Changed Talk given at the Gray Institute in 2015
The inspiration for sharing this story comes from the book I’m currently obsessed with. Everything is Figureoutable, by Marie Forleo.
It stands to reason that if you feel stiff every morning, you ought to stretch yourself out. Don’t waste time feeling old or pining for the days you could jump out of bed without giving you body a second thought. Just stretch it out.
The vast majority of muscle aches and joint pain can be worked out with a combination of mindset and movement. If you are sore you aren’t broken. Your body is craving something different and nothing good will happen until something changes.
Choose to do something different and be consistent with it. If you aren’t sure where to begin, try this or some variation of it.
Knee pain can stop you in your tracks. It also continues to be surprisingly mishandled by many healthcare practitioners. People with knee pain would do anything to be rid of it, so following a doctor’s advice for a cortisone (steroid) injection or two is often a no-brainer.
Unfortunately, there’s a problem with that.
Despite mounting evidence that they do no good, steroid injections are among the most common ‘treatments’ for knee pain. The research has been clear for years — steroid injections do not lead to good outcomes for joint pain. A 2017 Journal of American Medicine (JAMA) article raises the stakes and brings the Hippocratic Oath to mind — ‘do no harm’.
Numerous researchers have proven that steroid injections have a placebo effect at best. The 2017 JAMA article goes one crucial step further — the steroid injected into your joint causes your cartilage to degrade. That’s exactly the opposite of what we want.
Doctors at Tufts Medical Center in Boston did a two year blind study with two groups of patients with arthritic knee pain. They also had what’s called synovitis — a type of inflammation in the joint, verified by ultrasound. If anyone is going to respond to steroids, these people should.
Each group got injections every 12 weeks for 2 years. One group had saline (placebo) injected, the other a steroid. An MRI was done at the beginning, after one year, and again at the end.
The dismal results are no surprise to Physical Therapists, who often see these patients at some point in time after injections. In my 25 years as a PT, I’ve heard a version of these 12 words more times than I could possibly count, “It seemed to help for a little while, but it didn’t last.”
The results of the JAMA study should NOT be surprising to doctors who continue to inject. This information is widely circulated in journals.
Here are the conclusions of that revealing study:
For pain it was a net zero effect. No difference in pain between the two groups. Thanks to the placebo effect, both groups did experience some decrease in pain.
No difference in function in either group. No improvement in stiffness. No improvement in walking.
Remember, one group got the steroid, the other got saline.
There was one significant difference discovered between the two groups, and it’s bad news for the cortisone recipients.
The steroid group had definitively less cartilage in their knees after two years. That’s BAD. The steroids sped up the rate of arthritic changes. The saline group had no change in thickness — that’s GOOD.
This is exactly the opposite of what patients (I like to call them people) and their doctors would want to happen.
Will this 2017 JAMA study change the recommendations from doctors and surgeons who’ve been giving them for years? We could assume it should, but assumptions are dangerous.
A Google search for information on cortisone shots brings up the current Mayo Clinic recommendations:
There’s concern that repeated cortisone shots might cause the cartilage within a joint to deteriorate. So doctors typically limit the number of cortisone shots into a joint. In general, you shouldn’t get cortisone injections more often than every six weeks and usually not more than three or four times a year
The JAMA study was within those current guidelines of a shot every twelve weeks or four times a year.
My advice would be to simply ask your doctor what they think about this and other studies or find a good Physical Therapist to consult with first. All 50 states allow direct access between you and your Physical Therapist — meaning you don’t need a referral.
One last thing, in 2018, a year after the JAMA study was published, there was an increase in supply and demand of cortisone shots. According to MarketWatch: Cortisone Shots Market 2018 Receives a Rapid Boost in Economy due to High Emerging Demands with CAGR of 5.2% by Forecast to 2023
America acquires the first position in the market for cortisone shots owing to the rising prevalence of various types of allergies, arthritis, tendinitis, and others, and rising demand for corticosteroid injection in the U.S. According to the Center for Disease Control and Prevention, an estimated 78 million i.e. 26% of the U.S. adults aged 18 years or older are projected to have doctor-diagnosed arthritis by 2040. Additionally, the prevalence of tendinitis among athletes is found to be increasing from last few years in the U.S.
Despite years of researchers — and patients — telling us that cortisone injections don’t really do the job, the market tells a different story. They are being purchased in even higher quantities. They are still being given liberally and usually before any Physical Therapy. They are causing more harm than good.
We need to handle joint pain differently. We’ve been discussing the knee here, but the same goes for hips, shoulders, spine and any other joint that gets injected. All treatment and advice should be geared toward getting a good outcome for the person experiencing pain and difficulty.
Any practitioner helping you with joint pain should be looking at you when you talk (not checking boxes on their computer), listening and asking questions, watching you perform the tasks/movements that cause pain, strategically finding moves that don’t, and giving you new cues and habits to build into your day. Habits based on mindset and movement.
If your doctor is still giving cortisone injections, ask them why. Perhaps they have a convincing argument, I just haven’t heard one yet.
I understand now that no one else in the world knows what I should do.
I doubt that I am alone in feeling this feeling today.
The news of closures and precautions and viral pandemic are blazing across my phone, my watch, the tv, our dinner table, and in the eyes of everyone I meet.
The experts don’t know, the doctors, the therapists, the journalists, the authors, my friends, my kids, they don’t know. Because this level of global shut down has not happened in our lifetime — certainly not in mine.
Yet through all the unknowing, I feel a weird calm — except when I read the article on the front page to the New York Times this morning about two guys in Tennessee (along with thousands of others) who went out and bought 17,700 bottles of hand sanitizer and began to resell it for $70 a piece. That’s just gross.
But now I’m calm again, because Amazon and EBay have cut them off. Karma is real.
Calm is not the same as indifferent. I know people are in pain, in fear, and suffering. I know there is a world of unknown about to hit our finances, businesses, and bodies.
So what I’m going to do is stop looking for someone else to tell me the right thing to do. It’s clear that this is spreading and I don’t want to make it worse by pretending I know something about it that I don’t know.
I’m going to stop. Breathe. Be still. Listen. Do the next right thing.
As Glennon Doyle has beautifully written in Untamed:
HOW TO KNOW: Moment of uncertainty arises Breathe, turn inward, sink. Feel around for the Knowing. Do the next thing it nudges you toward. Let is stand. (Don’t explain.) Repeat forever. (For the rest of your life: Continue to shorten the gap between the Knowing and the doing.)
Why do some of us struggle with time, while others make it look so easy? We all have the same 24 hours in every day.
I like to keep things simple, so a good visual goes a long way for me.
Imagine you have a large glass jar. Next to it, you have a few large rocks, a small pile of marble sized pebbles, and a pile of sand. If you put in the sand or pebbles first, what happens? You can’t fit the big rocks in. But if you add the big rocks first, followed by the medium sized pebbles, and only then the sand, it all fits. (I got this from Tim Ferris, serial experimenter, podcaster, author, etc)
It’s a crystal clear reminder that the important things — the big rocks — come first. So why is it so easy to do the opposite? To get so focused and exasperated from dealing with the minutia that we repeat unhelpful mantras like:
“I’ll make time for that {important thing} tomorrow, or next week when it’s not so crazy, or next month after the Holidays, once this project is done, when I retire…”
The big rocks are the things that matter. In my personal life, that’s my kids, Nicole, the couple of handfuls of friends and family that I love and connect with, and my health. A positive state of health and wellbeing is the cornerstone for success in anything and everything. We can measure that health by our physical, emotional and social states.
If you are looking for the big rocks, start with your own personal state of the union.
Not sure how to put this into action? First, check your ‘personal state’ — your physical, emotional and social health. How does your body feel and are you moving enough and with some variety? Is your mind racing with schedules, worry, doubt, resentment and if so, what are you doing to quiet that fire? How are your relationships and are you nurturing the good ones or forcing the bad ones?
When your personal state is in the positive, the stories you tell yourself and others create a powerfully positive narrative. The opposite is true for when your story has shifted to the dark side. This internal and external narrative is the best barometer of what your state is at any given point. Use it to check yourself and to right yourself. It can be as simple as noticing when you are thinking and spewing negativity and deciding to stop.
The big rock visual works in business too. For me, the one thing I don’t want sitting outside my jar is customer service. We are a customer service company that happens to help people with pain, fitness, and performance. You can’t help people — in the way we seek to — without building relationships with them.
We measure our success by the personal state of our clients and by clearing the path for them to move better and feel better, so they have the freedom to do whatever they like. When you sift away the sand the the pebbles, it really is that simple.
In my consulting practice with people and organizations, we find the big rocks by asking questions to identify two things: what they really want (not always obvious), and what has gotten in the way of that. Once you recognize barriers, you have an opportunity to remove them. Often the gold is not found by adding more, but by taking away.
Here’s a recent example. When consulting for a non-profit in Boston, the issue at hand was an 80% participant drop out rate. The point of the organization is to make it easy for a specific group of people to get much needed, highly specialized, life saving services around PTSD.
I organized the research around my personal and professional experiences, asked a lot of layered questions, worked closely with the team on the front lines, and went to Boston to present my two cents. They were putting the sand and medium sized pebbles in the jar first and there was no room for the big rocks.
I did a customer on-boarding analysis, taking screenshots of my online registration process as if I were someone in their target audience attempting to sign up for the program directly from their website. This is a non-profit closely associated with a BIG hospital system. Someone made the call that all communications with even potential participants (the people they seek to serve) had to be ’secure’.
I presented the leadership with screenshots, of the 13 frustrating steps I had to go through in order to receive my first ‘welcome’ email from them. After all my trouble, the ‘welcome email’ was decidedly underwhelming. They had absolutely no idea this was happening to potential participants. The unintended consequence from that one decision to require ’secure’ communications was devastating to their mission.
I felt like Ralphie in the The Christmas Story when he worked his butt off to get his Little Orphan Annie Secret Decoder Ring, excitedly wrote down his first secret code, found the only place in the house he could get some privacy, and broke the code… only to reveal a crummy commercial: Be sure to drink your Ovaltine.
Back in Boston, there were three big problems with insisting on this ’secure’ policy so early on in the engagement process:
The people they are seeking to serve, by the nature of their circumstances, are easily frustrated and skeptical.
There was nothing confidential being shared, so a 13 step process to ensure the security of the impersonal ‘welcome email’ was overkill.
People in real need were dropping out before they even began.
Time, after all, is our only real commodity. They were wasting their own time by creating these inefficient and elaborate systems. Even worse, they were wasting precious time and patience of those they set out to support.
When things aren’t working — in life, work, relationships — it’s worth taking the time to dump out your jar and choose the biggest rocks first.
In Studio Sessions with a Licensed Physical Therapist
Pain, Fitness & Performance coaching with a Licensed Physical Therapist.
Are you struggling with nagging pain, tired & achy muscles, or an injury?
Do you know that exercise is important, but have trouble getting motivated or sticking with it?
Are you an athlete anxious to get back in the game?
For over 25 years, we've helped thousands of people like you sift through complex situations. We analyze your dynamic situation to give you the insights, choices, and action steps you need to live life on your terms.
3D MAPS Certified - Movement Analysis Performance System
Robin's Bio
Robin Dufour empowers people of all ages to overcome their struggles with recurring pain, fitness, and injury.
She approaches each situation with enthusiasm, persistence, and a keen sense of humor, crafting individualized and science-based programs for each person or group of people.
Her goal is to help individuals, families, and teams become experts in their physical wellbeing so they can enjoy a healthy balance in occupation, life, and play.
She loves being able to laugh and celebrate with clients as they overcome difficult situations and move beyond old limitations.
Special Interests:
Robin is often sought out to assist with challenging pain issues when other treatments have been unsuccessful. She is particularly skilled with seemingly complicated cases of recurring pain, discomfort, and aversion to regular exercise. She also specializes in resolving the causes of workplace injury.
Her experience as a parent, business owner, practitioner, and enthusiastic student of life offers a refreshing alternative to traditional physical therapy and fitness.
Robin loves spending time with her two daughters, her partner Nicole, and a handful of long-time friends - whom she credits for fine-tuning her sense of humor and humility.
She'll never pass up a walk on the beach, a great book, or a nice glass of wine in her spare time.
Experience & Training:
Following graduation from the University of New England in 1995, Robin became a licensed Physical Therapist. She opted for a series of challenging jobs in physical rehabilitation with neurologic injury, pediatrics, geriatrics, and sports medicine. She credits this diversity in finding common threads and practical solutions for a broad range of clients.
In 2010, she earned the distinction of Fellow of Applied Functional Science with the prestigious Gray Institute. She went on to become a five-year member of the faculty - teaching movement and health practitioners from around the world.
Robin has a particular interest in Veteran and Family care. In 2018-2019 she was hired as a special consultant for Home Base Veteran and Family Care. Home Base is a Red Sox Foundation and Massachusetts General Hospital Program dedicated to healing the invisible wounds for Veterans of all eras, Service Members, Military Families, and Families of the Fallen through world-class clinical care, wellness, education, and research.
At Home Base, Robin analyzed the existing program and recommended new ways to better serve more Veterans and Families in their Warrier Health and Fitness program in Boston and South West Florida.
Robin is an institutional health consultant, assessing past and current spending on musculoskeletal injuries - the highest cost in healthcare. In partnership with Solve Global, she identifies areas of risk in the workplace and provides measurable solutions for reducing spending and improving outcomes and culture.
She enjoys public speaking to engage audiences in the nuances of movement, mindset, and behavior as an alternative to pills and procedures.
Following her curiosities has led her to pursue local and national teaching opportunities. You can watch a sample of talks given at the Gray Institute here.
She has spent the last 25 years studying the art and science of the human body. Specifically, how we are affected by internal and external forces like gravity, mass and momentum, pain, joy, trauma, injury, receptive motions.
You name it, and we can be affected by it.
In recent years her studies and practice have led her to leave the clinical setting in favor of a more relaxed and creative environment. Five years ago, she left her beloved Studio Be in Maine to open Be Fit Co. in Williamstown, MA. If you like a good "stars aligning" story, ask her what led her to take that leap.